- Research
- Open access
- Published:
Predictors of depression among caregivers of children with malnutrition in Gedeo zone public hospitals, Southern Ethiopia: case-control study
BMC Psychiatry volume 25, Article number: 500 (2025)
Abstract
Background
Depression is a leading cause of disability worldwide, significantly impacting global health, particularly for women. It accounts for 4.3% of the total disability-adjusted life years (DALYs), making it a major contributor to global disability. The high rate of depression in developing nations, the caregiving responsibilities of caregivers, their susceptibility to depression, and maternal mental health in these nations may significantly impact childhood development. Therefore, the study aimed to identify the predictors of depression among caregivers of children with malnutrition in Gedeo Zone public hospitals.
Methods
A facility-based unmatched case-control study was conducted. A systematic sampling technique was used to select 226 caregivers (113 cases and 113 controls). Depression of caregivers was assessed using a patient health questionnaire (PHQ-9). Data were analyzed using SPSS version 20. Bivariate and multivariate logistic regression analysis was conducted to identify predictors, and the association was presented with an adjusted odds ratio and a 95% confidence interval.
Results
In this study, not attended formal education [AOR = 2.9(95%CI: 1.0-8.1)], unemployment [AOR = 3.7, (95% CI: 1.4–9.7)], low socioeconomic status [AOR = 3.3 (95% CI: 1.2–9.4)], physical abuse [AOR = 2.3(95% CI = 1.2–3.3)], poor social support [AOR = 2.6(95% CI: 1.0–6.5)], and stunting [AOR = 2.5, 95% CI: 1.3–3.4] were a significant positive predictors of depression.
Conclusion and recommendation
Nearly half of the study participants had a significant burden of depression among caregivers of malnourished children; particularly those facing not attended formal education, unemployment, low socioeconomic status, physical abuse, poor social support, and having a stunted child. Therefore, implementing early depression screening and interventions is crucial. Additionally, enhancing caregiver education, reducing unemployment, strengthening social support systems, preventing stunted physical growth, and boosting parents’ financial stability with malnourished children are essential strategies for sustainable improvement.
Introduction
Depression is a state of low mood and aversion to activity that can affect a person’s thoughts, behavior, feelings, and sense of well-being. People with depressed moods can also experience feelings of sadness, lack of interest, hopelessness, helplessness, worthlessness, guilty feelings, irritability, change in appetite, sleep disturbance, suicidal ideation, and attempts [1].
Depression accounts for 4.3% of the global burden of disease and is among the largest single causes of disability worldwide, particularly for women [2, 3]. The first year after birth carries a significant risk of depression for primary caregivers [4]. Depression in caregivers is one of today’s all-too-silent health crises [5]. Caregivers who are at risk for depression are almost three times higher than in the general population of similar age [6]. Worldwide, caregivers experience depression two to three times more than men [7]. Caregivers handle all aspects of a sick relative’s care, physical, emotional, medical, and financial. This leads to significant life changes for the caregiver [8].
The risk of depression in primary caregivers is higher, and women are also prone to the postpartum period because of hormonal changes associated with childbirth and stressors associated with parenting [9]. The vulnerability of caregivers to depression, their childcare responsibilities, and the high prevalence of depression in developing countries, maternal mental health in these countries could have a substantial influence on growth during childhood [10].
The nutritional state of children is significantly impacted by the mental health of the primary caregivers, which also interferes with the primary caregiver’s ability to provide childcare [11,12,13]. By impairing the primary caregiver’s capacity to deliver appropriate care and feeding, maternal sadness and depression can have a direct effect on a child’s nutritional condition. Moreover, poverty and food insecurity can worsen maternal distress and child undernutrition, creating a vicious cycle of risk factors with long-term consequences for both caregiver and child [12].
Studies from different countries found that caregivers of malnourished children have a higher depression rate than those of well-nourished children; as reported from Uganda, the prevalence of depression among caregivers of malnourished children was 42% compared to 12% among mothers of controls [14] Kenyan about 64.1% mother with malnourished children has depression higher than mothers of normal-weight children (5.1%) [15].
Malnutrition impairs physical growth, increases morbidity and mortality, and reduces cognitive development and physical work capacity [16]. Malnutrition is also an underlying risk factor that increases the morbidity and mortality of many diseases in children and adults [17]. This is a global public health crisis, imposing significant health and economic burdens worldwide. Each year, it claims the lives of 3.1 million children under the age of five and contributes to widespread malnutrition, resulting in 165 million stunted, 99 million underweight, and 51 million wasted children in 2012 alone [2]. Nearly 20 million children who live in South Asia and Sub-Saharan Africa (SSA) are severely and acutely malnourished [18]. From SSA, Ethiopia is the second highest country impacted by malnutrition according to the Ethiopian Mini Demographic and Health Survey (EMDHS) report. The prevalence of child stunting, underweight, and wasting was 42%, 9%, and 26.7%, respectively [19].
While dietary and environmental factors are known major contributors to children’s nutritional status, research suggests caregiver mental health can also be a significant factor, potentially impacting a mother’s ability to care for her child [11, 20, 21]. Psychosocial factors, including caregiver mental health status, affect breastfeeding in both high- and low-income countries [22,23,24]. Caregivers with depression symptoms also stop exclusive breastfeeding earlier than caregivers without symptoms [23, 25]. Low income, educational level, husbands’ infidelity, lack of financial support, age of a child, residence, region, mothers’ education level, sex of a child, and family size were the factors that predict caregivers’ depression [19, 26,27,28,29].
High-income countries reported the relationship between caregiver mental health and children’s long-term emotional, cognitive, and Behavioural issues; in low- and middle-income countries (LMIC), where stunted growth as a result of malnutrition is a significant issue, this relationship has received less attention [30,31,32]. However, caregiver mental health is sometimes overlooked in child health programs in underdeveloped nations; intervention programs to enhance caregiver mental health should be taken into consideration as a method to address child malnutrition [33]. Therefore, this study aimed to identify predictors of depression among caregivers having children with malnutrition.
Methods and materials
Study area, period, and design
An institution-based unmatched case-control study was conducted in Gedeo Zone, Southern Ethiopia, from March 12 to May 30, 2024. Gedeo zone is located in the Southern Ethiopia regional state, which is 360 km away from Addis Ababa, the capital city of Ethiopia. In the administrative center of Dilla town, there are 276 health facilities. Among the total health facilities, one is a referral hospital, three district hospitals, 38 health centers, and 36 private clinics.
Participants
All caregivers of children with malnutrition attending public hospitals in the Gedeo Zone during the study period were included. Cases were defined as caregivers of malnourished children who have depression (PHQ-9 score ≥ 10), while controls in this study are caregivers of malnourished children who do not have depression (PHQ-9 score < 10). In both groups, caregivers with severe comorbid illnesses or communication difficulties were excluded from the study.
Sample size determination
The sample size was calculated using the double population proportion formula and computed by using the STATCALC application of Epi-Info version 7 statistical software with the following assumptions: 95% CI, power of 80%, and assuming that 20% of controls had depression compared to 40% of cases [14]. This gave us a total sample of 209, with a control-to-case risk ratio is 1:2, and adding a 10% non-response rate. Thus, the sample size required for the study was 230(115 cases and 115 controls).
Sampling procedure
There are four public hospitals in the Gedeo zone, including Yirga Chefee, Bule, Gedeb Primary Hospital, and Dilla Teaching Hospital. During the data collection period, an average of 575 caregivers of malnourished children visited these hospitals in a month (142 from Yirga Chefee, 92 from Bule, 108 from Gedeb Primary Hospital, and 233 from Dilla Teaching Hospital). The sample size was allocated proportionally to these selected public health hospitals. The sampling interval, determined by dividing the total study population by the sample size, k = n/N, 575/230 = 2.5 ≈ 3. Based on this, participants were selected by including every 3 intervals from the sampling frame until the total sample size allocated for each hospital was reached. The starting point was randomly selected. Then, a systematic sampling technique was used to select all cases and controls. (Fig. 1)
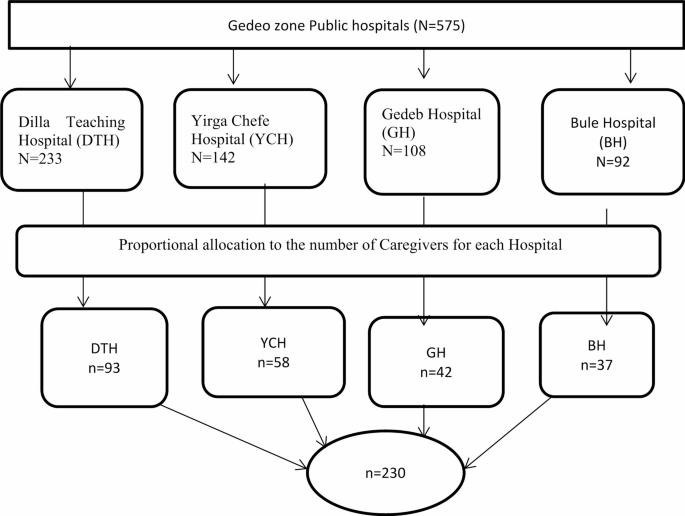
Showing sampling technique and procedure for predictors of depression among caregivers of malnutrition children in Gedeo Zone public Hospitals, in southern Ethiopia
Data collection instrument
Data was collected by reviewing the patient chart as well as using an interviewer-administered questionnaire, which was adapted to the local contexts employed as a tool for this study. The data were collected by four psychiatry nurses, and four nursing staff supervised by three mental health specialists. The questionnaire had different sections, including Socio-demographic, Caregivers’ characteristics, caregiver depression, perceived stigma, maternal workload, social support, Intimate partner violence, Wealth index, and Anthropometric measurement.
Socio-demographic characteristics
included residence, sex, age, marital status, ethnicity, religion, education, occupational status, and socioeconomic status.
Caregivers’ characteristics
individuals’ clinical characteristics, perceived stigma, social support, and substance-related factors were considered.
Caregivers’ depression
was assessed using the Patient Health Questionnaire-9 (PHQ-9) [34]. PHQ-9 score ranges from 0 to 27. Each of the 9 items was scored from 0 (not at all) to 3 (nearly every day) [34]. The PHQ-9 has been validated in Ethiopian studies for screening depression. In urban areas, a cut-off score of ≥ 10 indicates depression with a specificity of 67% and a sensitivity of 86%, respectively. However, in rural areas, a cut-off score of ≥ 10 indicates depression ≥ 5, with a sensitivity was 83.5% and a specificity was 74.7% [35, 36].
Perceived stigma
was assessed using a three-item stigma scale, which is validated in Zambia and comprises of dichotomous questions in which a positive response is indicative of perceived stigma with an overall possible score ranging from 0 (no perceived stigma) to 3 (maximally perceived stigma) [37].
Social support
was measured using the Oslo 3-item Social Support Scale (OSS-3) [38], which categorizes as follows: a score of 3–8 indicates poor social support, a score of 9–11 indicates intermediate social support, and a score of 12–14 indicates strong social support [39]. The Oslo-3 social support scale is a common tool in Ethiopian studies for screening the level of social support, in research concerning psychiatric disorders. A study conducted in Nigeria reported strong internal consistency for the Oslo-3 tool, with a Cronbach’s alpha of 0.91 [40].
Intimate partner violence
Women in a current or past intimate relationship were considered to have experienced intimate partner violence (IPV) in the past 12 months if they had suffered any of the following: sexual, psychological (emotional), or physical violence, or a combination of these [41].
Physical abuse
caregiver’s responses to seven survey questions regarding physical intimate partner violence (IPV) experienced in the last 12 months. The questions pertained to acts such as pushing/shoving, slapping, punching, kicking/dragging/beating, choking/burning, weapon use, and hair pulling/arm twisting.
Sexual abuse
Caregiver’s response to two survey questions- regarding experiences of sexual abuse in the past year, including being coerced into sexual intercourse or engaging in sexual acts without their consent in the last 12 months.
Emotional abuse
caregiver’s response to three survey questions- about being humiliated in front of others, threatened to hurt or harm someone close, or insulted in the last 12 months.
Wealth index
Household wealth index was assessed using the Principal component Analysis (PCA) [42]. The index was calculated based on selected household assets; ownership like (radios, mobile phones, beds, mattresses, kerosene lamps, watches, electric or solar panels, chairs, tables, wooden boxes, and carts were considered), materials utilized for the house construction like (uppermost cover, interior roof, floor, and walls) categorized by construction materials based on interviewer observations), and the size of agricultural land. National wealth quintiles are then created. This was done by assigning the highest based on their wealth score, and finally, household incomes were categorized into three Tertile household’s wealth score to every participant within that house. Then all participants are ranked lowest to, such as Low socioeconomic status (SES), Middle SES, and High SES [43].
Maternal workload
was assessed using the PCA [44], which was applied to ten activities performed by caregivers in the preceding 1 week of the survey and were included in the analysis. These activities included collecting firewood and fetching water (> 30-minute walk), washing clothes, land preparation, weeding, manual mowing, threshing, grinding/pounding grain, and terracing. The resulting components explained 70.6% of the variance and were used to classify caregivers into three workload categories (low, medium, and heavy).
Anthropometric measurement
Children’s ages and physical condition were recorded from patients’ charts, and mid-upper arm circumference (MUAC, weight, and height were taken following standard anthropometric procedures [45]. Anthropometric measures were converted into height for age, weight for height, and weight for age (underweight, stunted, and wasted, respectively). Finally, cases were considered if their Z scores were below minus three standard deviations (− 3SD) and a MUAC less than 115 mm according to WHO growth standard measurements [45].
Data quality control
Data were collected by reviewing patients’ charts and using the Amharic language, a semi-structured questionnaire, which included socio-demographic, depression, perceived stigma, social support, intimate partner violence, socioeconomic status, and maternal workload. Four psychiatry nurses and four nursing staff were recruited and trained for two days as data collectors at each selected hospital. Three supervisors (MSc in psychiatry) were involved during data collection time to supervise the overall data collection procedures. A pretest was conducted on 12 caregivers at a nearby district health center to check the instrument’s clarity. Based on the pretest findings, the questionnaire was revised. The English version of the questionnaire was translated into both Amharic and Gede-uffa and back-translated into English to ensure consistency. Collected data were checked daily for completeness and accuracy.
Data processing, analysis, and interpretation
First, the data was checked for completeness and consistency. The coded data were entered into Epi-Data version 3.1 and analyzed using SPSS Version 25. The nutritional status of children, such as anthropometric data, were calculated using WHO Anthro version 3.2 and categorized as stunted (height-for-age z-score < -3 SD, wasted (Weight-for-height z-score < -3 SD), and underweight (weight-for-age z-score < -3 SD), then, the data were exported to SPSS Version 25 for analysis. Data was presented by using text, frequencies, tables, charts, and figures. Bivariate and multivariate logistic regression analyses were performed to identify predictors. In the bivariable analysis, variables with p-values less than 0.2 were considered for inclusion in the multivariable analysis to control for potential confounding factors. A p-value less than 0.05 was considered statistically significant. The strength of the association was assessed using an adjusted odds ratio, and the presence of an association was presented with a 95% confidence interval. The model’s fitness was assessed, and the Hosmer-Lemeshow test yielded a p-value of 0.72. Tolerance and variance inflation factors (VIFs) were checked to evaluate multicollinearity; the tolerance was ≥ 0.268, while the VIF was ≤ 4.97.
Results
Socio-demographic characteristics of caregivers
From a total of 230 study participants, 226 completed the interview, yielding a response rate of 98.3%. The age range of the participants was between 19 and 42 years, with a mean age of 30.95 years (SD ± 5.5). Of this, nearly half (49.0%) of the caregivers were found in the age group of 25–34 years. Approximately 87 (42.6%) of caregivers had received formal primary education, and two-thirds (65.7%) of the participants were unemployed (Table 1).
Psychosocial and clinical characteristics of the caregiver
Regarding psychosocial aspects of caregivers with malnourished children, about 44.1% of study participants had inadequate social support. Nearly two-fifths of the study participants (39.7%) experienced intimate partner violence. Nearly half (48%) of participants reported experiencing perceived stigma as the caregivers of malnourished children. More than half (55.9%) of caregivers were dissatisfied with their marital relationship. About 17.6% of caregivers had a history of mental illness (Table 2).
Anthropometric measurements of children
Among children with malnutrition, approximately 75.5% were underweight, 62.3% were stunted, and 43.1% were wasted. Of the malnourished children, 21.9% had acute respiratory infection and 52.7% had diarrhea (Table 3).
Determinants of depression among caregivers of children with malnutrition
The associations of all potential explanatory variables and depression were checked using a logistic regression model. Not attending formal education, being unemployed, poor economic status, physical abuse, poor social support, heavy maternal workload, and stunting physical growth were significantly associated with depression, both in bivariate and multivariate logistic regression, with p-value < 0.05. (Table 4).
Discussion
Depression can exert a negative influence on a child’s nutritional intake by impeding social interaction and responsiveness. Depressed caregivers may experience challenges in fulfilling the demands of caregiving, potentially resulting in diminished engagement with their child and consequently impacting the child’s physical growth.
In the current study, we assessed possible predictors of depression among caregivers of children with malnutrition.
Caregivers with children who did not attend formal education were 2.9 times more likely to experience depression. This finding is in line with studies in Ethiopia, Botswana, Saudi Arabia, and Japan [46,47,48,49,50]. Poor reading skills can extend to emotional and behavioral problems, consequently increasing an individual’s vulnerability to depression and hindering their ability to manage their symptoms effectively [51]. Limited literacy can contribute to low self-esteem, reduced confidence in decision-making, and feelings of burden, especially when caregivers face challenges. This, combined with the economic strain often associated with lower education levels, can increase stress and the risk of depressive symptoms [52]. Unemployed caregivers were 3.7 times more likely to experience depression compared to caregivers who were employed. This finding is in line with studies in Sudan, Kenya, and Saudi Arabia [47, 53,54,55]. Unemployed caregivers may experience psychological distress and anxiety due to concerns about finding work, financial hardship, and lack of income. This unemployment can further exacerbate stress and contribute to depression, especially during the postpartum period [56].
Caregivers with low socioeconomic status were 3.3 times more likely to experience depression compared to caregivers with high socioeconomic status. This finding is in line with studies in Ethiopia, Kenya, India, Pakistan, and Uganda [26, 49, 57,58,59,60]. Living in low socioeconomic settings can create a persistent cycle of stress. Financial insecurity, difficulty affording basic needs, and unstable housing can all contribute to the development of depression in caregivers. This constant pressure affects their emotional well-being and limits their choices in housing, employment, and childcare, leaving them feeling powerless [52, 61, 62].
Caregivers with poor social support were 2.6 times more likely to experience depression than caregivers with strong social support. This finding is in line with studies in Ethiopia [50, 55, 63,64,65], Sudan, Pakistan, and Japan. The possible reason might be caregivers with a lack of social support are more susceptible to stress, loneliness, hopelessness, low self-esteem, and psychological distress [66].
Caregivers with a heavy workload were 2.1 times more likely to experience depression compared to caregivers with a low workload. Heavy workload is considered a factor contributing to distress and depression. the workload is a major contributor to stress and mental health issues like depression symptoms, feelings of helplessness, and hopelessness [67]. An excessive workload can lead to burnout, a state of emotional, physical, and mental exhaustion caused by prolonged or excessive stress. Burnout can make it difficult to concentrate, feel motivated, and complete tasks, further worsening the situation [68, 69].
Caregivers with children who were stunted were 2.53 times more likely to experience depression compared to mothers of children who were not stunted. This is in agreement with studies done in Ethiopia, Kenya, Uganda, Botswana, India, and Pakistan [26, 48, 50, 57, 70, 71]. Caregivers of stunted children face unique stressors related to their child’s health and development. These stressors, coupled with feelings of helplessness, sadness, and low self-esteem, can significantly impact their well-being [13].
Caregivers who experienced physical abuse were 2.33 times more likely to develop maternal depression compared to mothers who did not experience intimate partner violence. This finding is supported by studies done in Bangladesh, and India [72, 73]. Physical abuse leaves deep scars. It increases the risk of depression by triggering feelings of helplessness, low self-esteem, and trauma. These experiences can leave survivors feeling hopeless, worthless, and deeply saddened all hallmarks of depression. Physical abuse can severely impact mental well-being, potentially leading to depression. Victims may struggle with feelings of worthlessness, hopelessness, and difficulty managing emotions, all of which can contribute to depression [72, 74,75,76,77,78].
Limitations
In this study, we identified the cause-and-effect relationships of depression among caregivers of children with undernutrition.
Depressive symptoms data were assessed based on maternal recall of the 2 weeks before the survey and may reflect under-reporting or over-reporting of depressive symptoms. The Data were assessed face to face interviews, so there might be response bias.
Conclusion and recommendation
In this study, we found factors contributing to caregivers’ depression among children with malnutrition. The distribution of depression among caregivers with malnourished children was high among caregivers with a lack of formal education, unemployment, poor social support, low economic status, a heavy workload, Physical abuse, and stunting in physical growth in children with undernutrition. Therefore, early screening and detection of caregivers’ depression are crucial and implementing community-based education programs to improve literacy and health awareness. Local governments and NGOs should integrate mental health education into existing caregiver, maternal, and child health programs. Educated caregivers are better equipped to seek help, understand nutritional needs, and support their children’s development, thereby reducing unemployment and improving socioeconomic conditions. To prevent physical abuse and strengthen social support, it is essential to establish community-based support groups and counseling services for caregivers affected by domestic violence. Additionally, healthcare and social workers should receive training to screen for depression and abuse during pediatric malnutrition visits. Addressing stunting in children requires a holistic approach that integrates targeted mental health services with proper child feeding practices. Combining psychological support and medical care ensures more effective interventions. Furthermore, supporting caregivers’ mental well-being enhances their adherence to nutritional guidelines, which promotes better physical and cognitive development in children.
For Policymakers
-
1.
Integrate mental health support into nutrition programs (e.g., adding counseling services to community malnutrition initiatives).
-
2.
Expand social protection programs like job training for families with malnourished children.
Data availability
The data included in the manuscript can be obtained from the corresponding author through the email address biazinyenealem21@gmail.come with rational request.
Abbreviations
- AOR:
-
Adjusted odds ratio
- CI:
-
Confidence interval
- COR:
-
Crude odds ratio
- EPDS:
-
Edinburgh Postnatal Depression Scale
- Epi-Data:
-
Epidemiological Data
- LMIC:
-
Low- and middle-income countries
- PHQ:
-
Patient Health Questionnaire
- PCGs:
-
Primary Care Givers
References
Al-Balushi N, Al Shekaili M, Al-Alawi M, Al-Balushi M, Panchatcharam SM, Al-Adawi S. Prevalence and predictors of depressive symptoms among caregivers of children with attention-deficit/hyperactivity disorder attending a tertiary care facility: a cross-sectional analytical study from Muscat, Oman. Early Child Dev Care. 2019;189(9):1515–24.
Black RE, Victora CG, Walker SP, Bhutta ZA, Christian P, De Onis M, Ezzati M, Grantham-McGregor S, Katz J, Martorell R. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet. 2013;382(9890):427–51.
Bauermeister JJ, Puente A, Martínez JV, Cumba E, Scándar RO, Bauermeister JA. Parent perceived impact of Spaniard boys’ and girls’ inattention, hyperactivity, and oppositional defiant behaviors on family life. J Atten Disord. 2010;14(3):247–55.
Kessler RC. Epidemiology of women and depression. J Affect Disord. 2003;74(1):5–13.
Alliance FC. Fact sheet: Selected caregiver statistics. San Francisco, CA: Family Caregiver Alliance Retrieved October 2001, 19:2011.
Schulz R, Tompkins CA, Rau MT. A longitudinal study of the psychosocial impact of stroke on primary support persons. Psychol Aging. 1988;3(2):131.
Union A. Protocol to the African Charter on Human and People’s Rights on the Rights of Women in Africa. 2003.
Paula CS, Lauridsen-Ribeiro E, Wissow L, Bordin IA, Evans-Lacko S. How to improve the mental health care of children and adolescents in Brazil: actions needed in the public sector. Revista Brasileira De Psiquiatria. 2012;34(3):334–51.
Gale S, Harlow BL. Postpartum mood disorders: a review of clinical and epidemiological factors. J Psychosom Obstet Gynecol. 2003;24(4):257–66.
Wachs TD. Models linking nutritional deficiencies to maternal and child mental health. Am J Clin Nutr. 2009;89(3):S935–9.
Rayhan MI, Khan MSH. Factors causing malnutrition among under five children in Bangladesh. Pak J Nutr. 2006;5(6):558–62.
Stewart RC. Maternal depression and infant growth–a review of recent evidence. Matern Child Nutr. 2007;3(2):94–107.
Surkan PJ, Kennedy CE, Hurley KM, Black MM. Maternal depression and early childhood growth in developing countries: systematic review and meta-analysis. Bull World Health Organ. 2011;89(8):607–15.
Ashaba S, Rukundo GZ, Beinempaka F, Ntaro M, LeBlanc JC. Maternal depression and malnutrition in children in Southwest Uganda: a case control study. BMC Public Health. 2015;15(1):1303.
Haithar S, Kuria M, Sheikh A, Kumar M, Vander Stoep A. Maternal depression and child severe acute malnutrition: a case-control study from Kenya. BMC Pediatr. 2018;18(1):289.
Pelletier DL, Frongillo EA. Changes in child survival are strongly associated with changes in malnutrition in developing countries. J Nutr. 2003;133(1):107–19.
Murray CJ, Lopez AD. Global mortality, disability, and the contribution of risk factors: global burden of disease study. Lancet. 1997;349(9063):1436–42.
Collins S. Changing the way we address severe malnutrition during famine. Lancet. 2001;358(9280):498–501.
Endris N, Asefa H, Dube L. Prevalence of malnutrition and associated factors among children in rural Ethiopia. Biomed Res Int 2017, 2017.
Black MM, Baqui AH, Zaman K, Arifeen SE, Black RE. Maternal depressive symptoms and infant growth in rural Bangladesh. Am J Clin Nutr. 2009;89(3):S951–7.
Surkan PJ, Kennedy CE, Hurley KM, Black MM. Maternal depression and early childhood growth in developing countries: systematic review and meta-analysis. Bull World Health Organ. 2011;89:607–15.
de Jager E, Skouteris H, Broadbent J, Amir L, Mellor K. Psychosocial correlates of exclusive breastfeeding: a systematic review. Midwifery. 2013;29(5):506–18.
Hasselmann MH, Werneck GL, Silva, CVCd. Symptoms of postpartum depression and early interruption of exclusive breastfeeding in the first two months of life. Cadernos De Saude Publica. 2008;24:s341–52.
Ystrom E. Breastfeeding cessation and symptoms of anxiety and depression: a longitudinal cohort study. BMC Pregnancy Childbirth. 2012;12(1):36.
Rahman A, Hafeez A, Bilal R, Sikander S, Malik A, Minhas F, Tomenson B, Creed F. The impact of perinatal depression on exclusive breastfeeding: a cohort study. Matern Child Nutr. 2016;12(3):452–62.
Rahman A, Iqbal Z, Bunn J, Lovel H, Harrington R. Impact of maternal depression on infant nutritional status and illness: a cohort study. Arch Gen Psychiatry. 2004;61(9):946–52.
DE MIRANDA CT, Turecki G, Mari JJ, Andreoli SB, Marcolim MA, Goihman S, Puccini R, Strom BL, Berlin JA. Mental health of the mothers of malnourished children. Int J Epidemiol. 1996;25(1):128–33.
Madeghe BA, Kimani VN, Vander Stoep A, Nicodimos S, Kumar M. Postpartum depression and infant feeding practices in a low income urban settlement in Nairobi-Kenya. BMC Res Notes. 2016;9(1):506.
Motlhatlhedi K, Setlhare V, Ganiyu AB, Firth JA. Association between depression in carers and malnutrition in children aged 6 months to 5 years. Afr J Prim Health Care Family Med. 2017;9(1):1–6.
Haas JD, Murdoch S, Rivera J, Martorell R. Early nutrition and later physical work capacity. Nutr Rev. 1996;54(2):S41.
Victora CG, Adair L, Fall C, Hallal PC, Martorell R, Richter L, Sachdev HS. Maternal, group CUS: maternal and child undernutrition: consequences for adult health and human capital. Lancet. 2008;371(9609):340–57.
Pollitt E, Gorman KS, Engle PL, Rivera JA, Martorell R. Nutrition in early life and the fulfillment of intellectual potential. J Nutr. 1995;125(suppl4):S1111–8.
Patel V, Rahman A, Jacob K, Hughes M. Effect of maternal mental health on infant growth in low income countries: new evidence from South Asia. BMJ. 2004;328(7443):820–3.
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–13.
Gelaye B, Williams MA, Lemma S, Deyessa N, Bahretibeb Y, Shibre T, Wondimagegn D, Lemenhe A, Fann JR, Vander Stoep A. Validity of the patient health questionnaire-9 for depression screening and diagnosis in East Africa. Psychiatry Res. 2013;210(2):653–61.
Hanlon C, Medhin G, Selamu M, Breuer E, Worku B, Hailemariam M, Lund C, Prince M, Fekadu A. Validity of brief screening questionnaires to detect depression in primary care in Ethiopia. J Affect Disord. 2015;186:32–9.
Baskind R, Birbeck GL. Epilepsy-associated stigma in sub-Saharan Africa: the social landscape of a disease. Epilepsy Behavior: E&B. 2005;7(1):68–73.
Bøen H. Social Support, mental health and effectiveness of a senior centre programme for elders living at home. Cross-sectional studies and a randomized controlled trial. 2012.
Bøen H, Dalgard OS, Bjertness E. The importance of social support in the associations between psychological distress and somatic health problems and socio-economic factors among older adults living at home: a cross sectional study. BMC Geriatr. 2012;12:1–12.
Dalgard O. Social\ support\-Consequences\ for\ individual\ and\ society\.\ EUPHIX,\ EUphact\ Bilthoven:\ RIVM,<\ http://www\ euphix\ org > EUphact\Determinants\ of\ health\Environment\Social\ support\ 2009,\ 16\.
Stöckl H, March L, Pallitto C, Garcia-Moreno C. Intimate partner violence among adolescents and young women: prevalence and associated factors in nine countries: a cross-sectional study. BMC Public Health. 2014;14:1–14.
Vyas S, Kumaranayake L. Constructing socio-economic status indices: how to use principal components analysis. Health Policy Plann. 2006;21(6):459–68.
Krishnan V. Constructing an area-based socioeconomic index: A principal components analysis approach. Edmonton, Alberta: Early Child Development Mapping Project 2010.
KebedeGebre K. Principal component analysis of birth weight of child, maternal pregnancy weight and maternal pregnancy body mass index: A multivariate analysis. Am J Theoretical Appl Stat. 2021;10(1):63–71.
Group WMGRS, de Onis M. WHO child growth standards based on length/height, weight and age. Acta Paediatr. 2006;95:76–85.
Matsumura K, Hamazaki K, Tsuchida A, Kasamatsu H, Inadera H. Education level and risk of postpartum depression: results from the Japan environment and children’s study (JECS). BMC Psychiatry. 2019;19:1–11.
Alzahrani J, Al-Ghamdi S, Aldossari K, Al-Ajmi M, Al-Ajmi D, Alanazi F, Aldossary A, Alharbi A. Postpartum depression prevalence and associated factors: an observational study in Saudi Arabia. Medicina. 2022;58(11):1595.
Firth JA, Motlhatlhedi K, Ganiyu AB, Setlhare V. Association between depression in carers and malnutrition in children aged 6 months to 5 years. Afr J Prim Health Care Family Med. 2017;9(1):1–6.
Endris N, Asefa H, Dube L. Prevalence of malnutrition and associated factors among children in rural Ethiopia. Biomed Res Int. 2017;20171:6587853.
Yenealem B, Negash M, Madoro D, Molla A, Nenko G, Nakie G, Getnet B. Prevalence and associated factors of maternal depression among mothers of children with undernutrition at comprehensive specialized hospitals in Northwest Ethiopia in 2023: a cross– sectional study. Front Psychiatry. 2024;15:1400293.
Maughan B, Carroll J. Literacy and mental disorders. Curr Opin Psychiatry. 2006;19(4):350–4.
Lorant V, Deliège D, Eaton W, Robert A, Philippot P, Ansseau M. Socioeconomic inequalities in depression: a meta-analysis. Am J Epidemiol. 2003;157(2):98–112.
Hummel AD, Ronen K, Bhat A, Wandika B, Choo EM, Osborn L, Batra M, Kinuthia J, Kumar M, Unger JA. Perinatal depression and its impact on infant outcomes and maternal-nurse SMS communication in a cohort of Kenyan women. BMC Pregnancy Childbirth. 2022;22(1):1–16.
Mabyoue MOE. Prevalence of post-partum depression among Sudanese women using Edinburgh postnatal depression scale (EPDS) in two major delivery hospitals in Khartoum state. Sudan J Med Sci. 2020;15(4):355–70.
Mekuriaw BY, Getnet B, Seid E, Teferi T, Alemwork A, Aschale M, Tsega A. Prevalence and associated factors of psychological distress among caregivers of children with malnutrition: a cross–sectional study. BMC Public Health. 2025;25(1):505.
Wake GE, Fitie GW, Ashenafi B, Tadese M, Tessema SD. Magnitude and determinant factors of postpartum depression among mothers attending their postnatal and vaccination services at public health institutions of addis Ababa, Ethiopia. Front Public Health 2022, 10.
Haithar S, Kuria M, Sheikh A, Kumar M, Vander Stoep A. Maternal depression and child severe acute malnutrition: a case-control study from Kenya. BMC Pediatr. 2018;18:1–9.
Anoop S, Saravanan B, Joseph A, Cherian A, Jacob K. Maternal depression and low maternal intelligence as risk factors for malnutrition in children: a community based case-control study from South India. Arch Dis Child. 2004;89(4):325–9.
Ashaba S, Rukundo GZ, Beinempaka F, Ntaro M, LeBlanc JC. Maternal depression and malnutrition in children in Southwest Uganda: a case control study. BMC Public Health. 2015;15:1–6.
Ross J, Hanlon C, Medhin G, Alem A, Tesfaye F, Worku B, Dewey M, Patel V, Prince M. Perinatal mental distress and infant morbidity in Ethiopia: a cohort study. Archives Disease Childhood-Fetal Neonatal Ed. 2011;96(1):F59–64.
Gundersen C, Lohman BJ, Garasky S, Stewart S, Eisenmann J. Food security, maternal stressors, and overweight among low-income US children: results from the National health and nutrition examination survey (1999–2002). Pediatrics. 2008;122(3):e529–40.
Verbeek T, Bockting CL, Beijers C, Meijer JL, van Pampus MG, Burger H. Low socioeconomic status increases effects of negative life events on antenatal anxiety and depression. Women Birth. 2019;32(1):e138–43.
Abadiga M. Magnitude and associated factors of postpartum depression among women in Nekemte town, East Wollega zone, West Ethiopia, 2019: A community-based study. PLoS ONE. 2019;14(11):e0224792.
Shitu S, Geda B, Dheresa M. Postpartum depression and associated factors among mothers who gave birth in the last twelve months in Ankesha district, Awi zone, North West Ethiopia. BMC Pregnancy Childbirth. 2019;19(1):1–9.
Deribachew H, Berhe D, Zaid T, Desta S. Assessment of prevalence and associated factors of postpartum depression among postpartum mothers in Eastern zone of Tigray. Eur J Pharm Med Res. 2016;3(10):54–60.
Lakey B, Cronin A. Low social support and major depression: research, theory and methodological issues. Risk Factors Depress 2008:385–408.
Greenglass ER, Burke RJ, Moore KA. Reactions to increased workload: effects on professional efficacy of nurses. Appl Psychol. 2003;52(4):580–97.
Rajan D. Negative impacts of heavy workload: a comparative study among sanitary workers. Sociol Int J. 2018;2(6):465–74.
Dominado NL, Valdez LG. Stress in the workplace, depression, and academic workloads of public school teachers. Int J Multidisciplinary: Appl Bus Educ Res. 2021;2(5):417–23.
Upadhyay AK, Srivastava S. Effect of pregnancy intention, postnatal depressive symptoms and social support on early childhood stunting: findings from India. BMC Pregnancy Childbirth. 2016;16:1–14.
Anato A, Baye K, Stoecker B. Determinants of depressive symptoms among postpartum mothers: a cross-sectional study in Ethiopia. BMJ Open. 2022;12(9):e058633.
Rahman M, Poudel KC, Yasuoka J, Otsuka K, Yoshikawa K, Jimba M. Maternal exposure to intimate partner violence and the risk of undernutrition among children younger than 5 years in Bangladesh. Am J Public Health. 2012;102(7):1336–45.
Ackerson LK, Subramanian S. Domestic violence and chronic malnutrition among women and children in India. Am J Epidemiol. 2008;167(10):1188–96.
Lindert J, von Ehrenstein OS, Grashow R, Gal G, Braehler E, Weisskopf MG. Sexual and physical abuse in childhood is associated with depression and anxiety over the life course: systematic review and meta-analysis. Int J Public Health. 2014;59:359–72.
Radell ML, Abo Hamza EG, Daghustani WH, Perveen A, Moustafa AA. The impact of different types of abuse on depression. Depress Res Treat. 2021;2021(1):6654503.
Li Y, Long Z, Cao D, Cao F. Maternal history of child maltreatment and maternal depression risk in the perinatal period: A longitudinal study. Child Abuse Negl. 2017;63:192–201.
Shay NL, Knutson JF. Maternal depression and trait anger as risk factors for escalated physical discipline. Child Maltreat. 2008;13(1):39–49.
Sørbø MF, Grimstad H, Bjørngaard JH, Lukasse M, Schei B. Adult physical, sexual, and emotional abuse and postpartum depression, a population based, prospective study of 53,065 women in the Norwegian mother and child cohort study. BMC Pregnancy Childbirth. 2014;14:1–9.
Acknowledgements
The authors of this study would like to acknowledge the participants of the study, the data collectors, the supervisors, and the staff members of the pediatric Department.
Author information
Authors and Affiliations
Contributions
BY: Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Supervision; Project administration; Writing — original draft and Writing — review and editing. AM, TT, MN, MA, EH, and AT: Data curation; funding acquisition; investigation; methodology; supervision; project administration; writing—original draft and review and editing.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Institutional Review Board (IRB) of Dilla University, and it was to be conducted following the Declaration of Ethical Guidelines. A formal letter of permission was obtained from the Department of Psychiatry. Written informed consent form was obtained from each study participant after detailed explanations before the interviews. The privacy of study participants and the confidentiality of the information were maintained during the data collection process. The collected data were used only for the objective of this study.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Mekuriaw, B.Y., Molla, A., Negash, M. et al. Predictors of depression among caregivers of children with malnutrition in Gedeo zone public hospitals, Southern Ethiopia: case-control study. BMC Psychiatry 25, 500 (2025). https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s12888-025-06959-1
Received:
Accepted:
Published:
DOI: https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s12888-025-06959-1